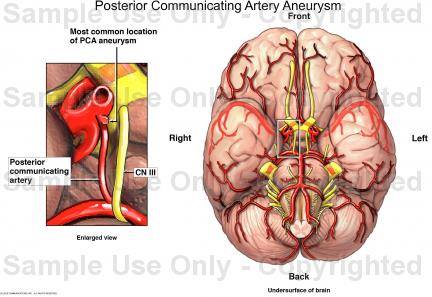
3rd nerve palsy due to Aneurysm of the POSTERIOR COMMUNICATING ARTERY
THE 3RD NERVE lies very close to the POST. COMM. ART. on the ventral (front facing) surface of the brainstem (specifically the midbrain because thats where the nucleus lies for the third nerve)
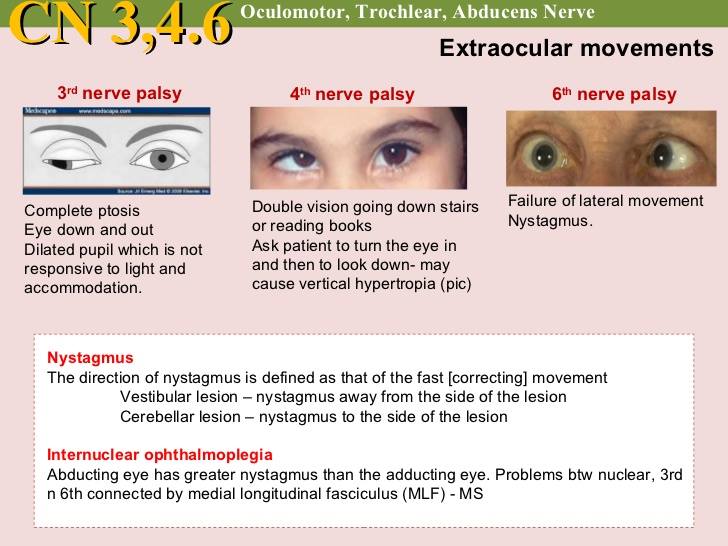
The third nerve or the OCULOMOTOR NERVE is the motor supply to ALL the extra ocular muscles of the eye EXCEPT LATERAL RECTUS (6 NV) and that crazy muscle the SUPERIOR OBLIQUE [SO] with the crazy nerve ( 4 NV )*
Lesion of the 3nv causes DOWN and OUT movement of the eye (down because SO takes over and out because LR takes over.)
Ptosis - levator palpebrae
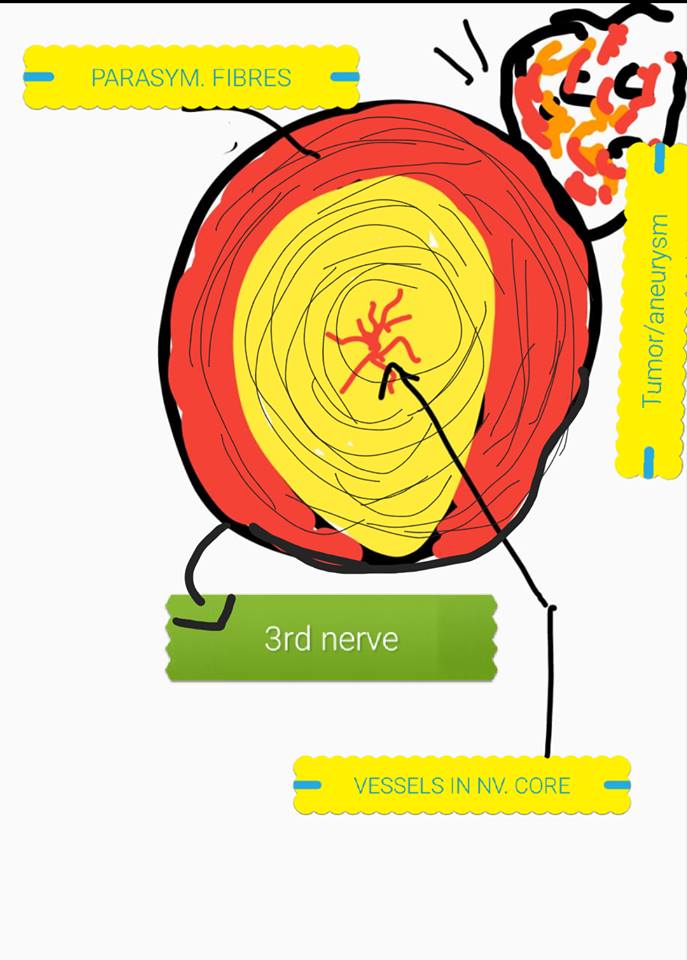
Pupil DILATION > parasympathetic fibres TO pupilliary muscles travel via the 3 nv. **
Now the interesting bit is… that in the 3 nv the PARASYMPATHETIC fibres travel on the OUTSIDE, so on compression from outside, be it tumor or aneurysm, the PARASYMPATHETIC fibres get affected first. Uh oh. Bad news. Patient presents initially with dilated pupil and gradually as the tumor or aneurysm grows the main bulk of the nerve gets effected , pressing on the vasculature present in the CENTRE of the nerve and effecting the motor function eventually. So lesion is moving from outside to inside.
On the other hand, diseases that effect the vasulature such as HTN VASCULITIS DM… they cause damage to the main bulk of the nerve causing MOTOR LOSS first then goes on further to effect the parasympathetic fibres on the outside. So the lesion is moving inside to outside.
In POST COMM ART. ANEURYSM… patient will INITIALLY have dilated pupil…then with growing size >>> Down and out eye (Diplopia) plus ptosis (drooping top lid)
IPSILATERAL lesion.
- the only stupid nerve that crosses over! Rest all other nerves travel on the same side!
** the pupilliary reflex centre is the EDINGER WESTPHAL nucleus which also lies in the midbrain. Parasympathetic centre causing CONSTRICTION normally.
Superior oblique is the reading and going downstairs muscle.