Investigations of RCM:
> Laboratory tests: Haemoglobin, WBC, serum iron and ferritin, liver, renal, and thyroid function tests, and serum electrolytes should be taken at initial assessment.
> Chest X-ray: reveals a normal cardiac size with possible atrial enlargement. Pulmonary congestion and pleural effusions may be present.
> ECG: shows non-specific ST-T changes with or without conduction abnormalities. The absence of increased voltage on ECG, despite the appearance of echocardiographic hypertrophy, can be the first clue to certain infiltrative diseases.
Low voltage and prolonged PR interval and a pseudoinfarction pattern in the inferoseptal wall are typical signs of advanced amyloidosis.
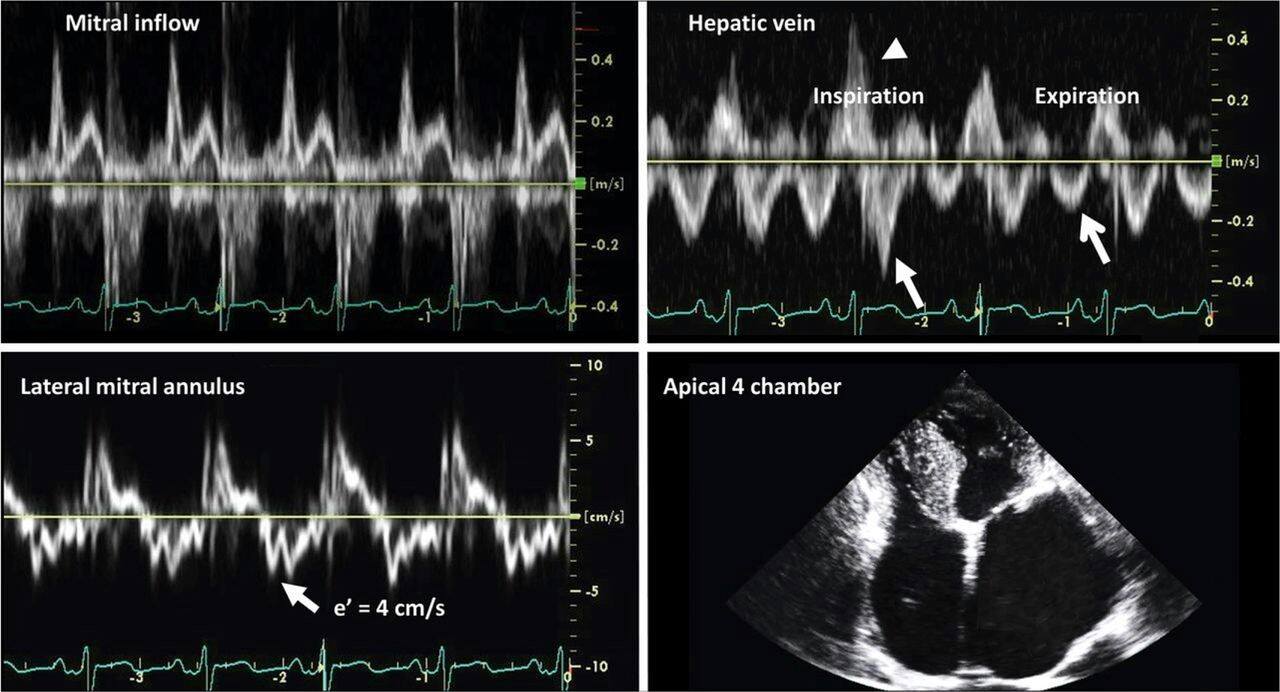
> Two-dimensional echocardiography Ventricles are small, with normal or increased wall thickness, and the atria are usually dilated. Valvular regurgitation and atrial enlargement are more common in RCM than in constrictive pericarditis.
Doppler echocardiography The pattern of mitral inflow velocity reveals increased early diastolic filling velocity (E wave ≥1 m/s), decreased late filling velocity (A wave ≤0.5 m/s), increased E/A ratio (≥2), decreased deceleration time (≤150 ms), and decreased isovolumic relaxation time (≤70 ms).
> Cardiac magnetic resonance has a higher resolution than echocardiography and detects the presence of myocardial fibrosis. It is particularly useful in the diagnosis of infiltrative diseases such as sarcoidosis, amyloidosis, radiation-induced fibrosis, iron loaded cardiomyopathy, and constrictive pericarditis.