Medicine takes to the air to serve far-flung populations
Called the mountain kingdom, Lesotho is the only country in the world situated entirely at elevations above 5,000 feet. It is an enclave, a small island floating within South Africa, its more developed neighbor. Although its rocky perch isolates the nation in many ways, in at least one sense, Lesotho is not alone: Like far too many countries, it struggles to provide its people with access to health care.
“On the day we arrived to survey the clinic site,” says Jennifer Furin ’99, an HMS assistant professor of medicine, “there were at least 25 people waiting. Yet there was no physician or nurse. So the Ministry of Health doctor and I sat down and began seeing patients. I think at least five people would have died that day had we not been there.”

Physician Jennifer Furin tends to a patient in Nohana.
The clinic Furin describes can be reached only by airplane, usually a single-engine Cessna that begins its flight at Moshoeshoe military airfield in Maseru, Lesotho’s bustling capital, and ends it an hour later in the mountain village of Nohana. Medical teams that arrive on the unpaved airstrip must carry their bags and crates of supplies on the 20-minute trek to the clinic.
“It’s no exaggeration to say the clinics are remote,” says Furin, the former medical director for the Partners In Health (PIH) program in Lesotho. “It’s like being on another planet. There’s no electricity and no cell phone coverage. It’s like being transported back in time—not to a good time but to a time when life was very hard.”
Rough Terrain
According to a 2006 report by the World Health Organization, a global shortage of 4.3 million health workers has translated into a lack of access to care for more than a billion people. In addition, the UN Millennium Project estimates that 2 billion people, a third of the world’s population, lack access to essential medicines. In the poorest parts of Africa and Asia, that proportion climbs to half.
Lesotho is one of 57 countries considered by WHO to have a critical health worker shortage: There are, for instance, only about 80 physicians to care for 2 million people. In addition, nearly one quarter of the population is thought to be positive for HIV, ranking this nation third highest in HIV prevalence globally, according to the U.S. Agency for International Development. And Lesotho’s HIV epidemic permeates every corner, rural and urban, of the country. Says Furin, “Shepherds and subsistence farmers living in the countryside have the same rate of HIV infection found among people living in the capital.”
Lesotho also has one of the world’s highest rates of tuberculosis infection, with a majority of those infected also testing positive for HIV. To complicate matters further, nearly 1,000 people each year contract strains of tuberculosis that are resistant to all first-line drugs.
Road Trip
Salmaan Keshavjee, a tuberculosis specialist and an assistant professor of social medicine in the School’s Department of Global Health and Social Medicine, is no stranger to jumping on a plane to provide care to people in remote settings. “Where I work in Western Siberia,” he says, “there are parts of the region that remain unreachable by ground transportation for months each year.”

Salmaan Keshavjee
When Keshavjee joined Furin in Lesotho in 2006, the government had already set up seven clinics in isolated parts of the country and had partnered with a nonprofit group of pilots affiliated with Lesotho’s health service to deliver supplies to mountain clinics and to airlift the gravely ill to facilities better equipped to care for them. But the infrastructure needed to provide adequate, consistent health care, especially to severely ill patients in the most remote areas, was nonexistent.
Keshavjee found, for example, that the Nohana clinic had no full-time staff, and that there was no capacity for either speedy or sustained care of patients who were infected with HIV and multidrug-resistant tuberculosis.
Pixel Post
Lawrence Shulman ’75, chief medical officer and senior vice president for medical affairs at Dana–Farber Cancer Institute, confronted similar difficulties during his travels to provide cancer care to remote populations in Haiti and Rwanda.
“There is little infrastructure in Haiti or Rwanda to provide cancer care,” says Shulman. “There are no trained oncologists, and there is little capacity to perform a biopsy. Without a biopsy, processed and read, you can’t know a patient’s definitive diagnosis. And without that diagnosis, you have no hope of successfully treating a patient.”
Shulman and colleagues at Dana–Farber, Brigham and Women’s Hospital, and Children’s Hospital Boston are working with PIH to build cancer care infrastructure in Haiti, Rwanda, and Malawi.
Shulman recently headed up a team of ten Dana–Farber oncologists and oncology nurses that will help run the first national cancer-care training program in Rwanda. The team will share basic knowledge in cancer care and, through remote connections with Boston-based colleagues, will establish ties to improve the delivery of cancer care in that country. Technology is playing a major role in this project, as it does for similar efforts aimed at improving access to health care.
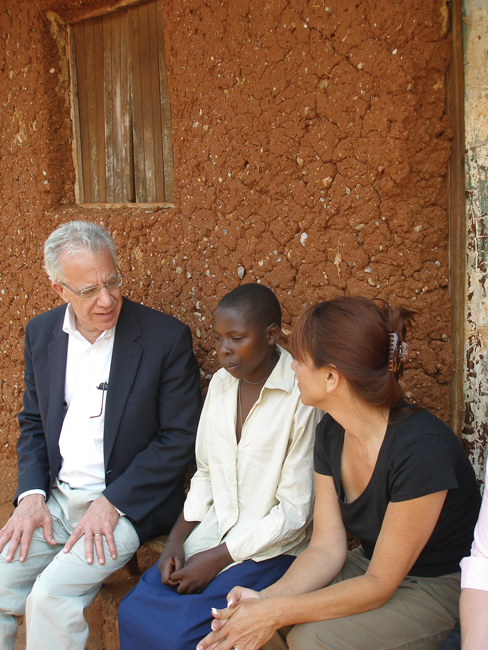
HOUSE CALLS: Lawrence Shulman (left) sits with a patient and colleague outside a clinic in Rwanda.
“Paul Farmer, as only he could do, took a picture with his iPhone of a blood smear from a patient with leukemia and sent the picture to me,” says Shulman. Farmer ’90, the Kolokotrones University Professor of Global Health and Social Medicine, heads the School’s Department of Global Health and Social Medicine. “The quality wasn’t very good,” Shulman adds, “but we were able to make the diagnosis and begin treatment. There are, of course, better ways to do this sort of thing, and we’re in the process of trying to figure them out.”
Picture Perfect
Keshavjee too is searching for better ways of using technology to deliver care to populations in remote areas. He describes the work of a female colleague in Pakistan who is developing simple strategies to monitor wound infections and other “visible” conditions. She hopes, for instance, to help keep post-operative patients free of infection by monitoring the status of surgical wounds through photos taken with mobile phones and then shared with wound specialists who help assess the healing process.
“It’s very expensive for poor patients to visit a doctor for a surgical wound check,” says Keshavjee. “But if you train health workers to take pictures of the wounds and then send those pictures to a doctor, many patients whose wounds are healing well could be saved the expense of a trip. If, however, the wound shows redness or the patient reports pain, the picture could be directed to a surgeon who could decide whether the person should travel to see a doctor.”
When faced with basic problems such as how to share medical records with other clinics or with the main office in Maseru, the Lesotho PIH team began using technology creatively. By installing an array of battery-backed solar panels, they provided the clinic with consistent power and communications access without expensive infrastructure, such as the signal transmission towers required by cell phones. They also arranged for access to two small communications satellites, links that allowed personnel in remote clinics to email the main office with requests for medications or supplies. Clinic administrators were also able to communicate better with the patient airlift service to schedule flights or to provide pilots with weather updates. In short, these uses of technology allowed clinic personnel to serve their patients better.
Tech Triage
What does the future hold? Keshavjee thinks the solution to improving access is to develop community-based, decentralized approaches that use technology tailored to help optimize care. And he sees this as a solution for all countries, not only developing nations.
Medical telecommuting would allow experts to consult on questions raised by health care workers traveling within rural or remote populations, says Keshavjee. And those populations could be in mountain clinics, or in inner cities. “In Boston,” he notes, “you see many people who are diabetic or who have high blood pressure. Often, they don’t see a doctor until they are hospitalized because of stroke or some other emergency.”

CAMERA READY: Village children gather to look at the images on the mobile phone of a health care worker. Patients visit a clinic in rural Rwanda (lower left).
A combination of community-based health workers and advanced technology would be an alternative to hospital-centric care, one that could achieve better health outcomes, especially for long-term disease management among people living in poor urban and rural areas.
“What if we could give diabetic patients cell phones with an app that allows them to enter their blood sugar values?,” asks Keshavjee. “A computer could flag patients whose glucose levels were off, a physician could evaluate those cases and, as needed, have a nurse call or a community health worker visit.” This approach, he adds, would not only be more effective, it could also save money by helping people avoid hospital stays and the repercussions of untreated disease.
“How can we link patients with care that can help them?” asks Keshavjee. “We can start by imagining all the ways technology can make distances smaller—and medical care more accessible.”